Humans take great pride in the fact that we dominate all other species with our sophisticated cognition. Yet while virtually all other species instinctively flee from smoke, we choose to suck it into our lungs. Worldwide, that one lapse in intelligence—inhaling tobacco smoke—costs us 6 million members of our species annually, while causing another 120 million or so to suffer from intractable lung, heart, and other diseases. Tobacco is now on pace to take one billion lives over the 21st century.
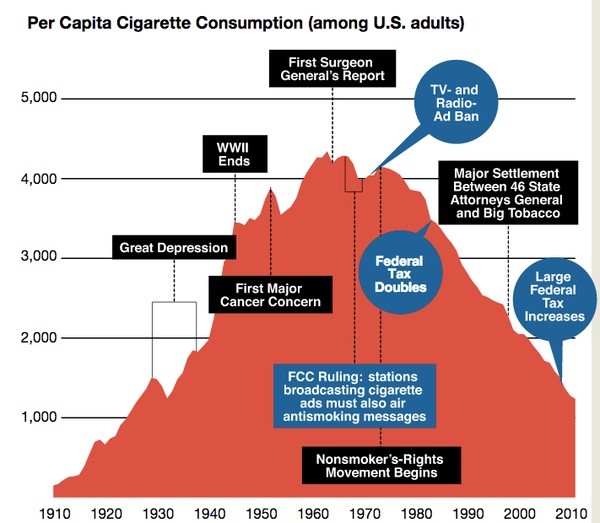
It’s hard to overstate the impact of this report. During the first six decades of the 20th century, smoking had grown from a casual pastime to a national addiction. In 1900, the average American adult smoked just 54 manufactured cigarettes each year. Then, in 1913, the R.J. Reynolds Tobacco Company introduced Camel cigarettes in what many consider to be the first modern advertising campaign. Shortly thereafter, cigarettes went to war. Before World War I, cigarettes were considered effeminate—manly men smoked cigars and pipes and used chewing tobacco. But in the trenches of Europe, soldiers did not have time to pack a pipe or savor a slow-burning cigar. Cigarettes were included in doughboys’ rations as they shipped off to Europe. Soldiers came home addicted to what Henry Ford called “the little white slaver.” Consumption increased rapidly after that, and by 1963, the average American was smoking 4,345 manufactured cigarettes per year.
Then, after Surgeon General Terry’s announcement, cigarette use suddenly began to decline. With only a handful of early exceptions, it has continued to decline annually ever since. Both the rise and fall of the cigarette were so dramatic that Harvard historian Allan Brandt dubbed the 1900s “The Cigarette Century.”
The 1964 report launched an era of tobacco control—a series of public- and private-sector interventions that, taken together, have averted an estimated 8 million premature American deaths. On average, each of these 8 million beneficiaries gained two full decades of life. It’s not hard to see why the Centers for Disease Control and Prevention included tobacco control on its list of 10 great public health achievements in the 20th century.
Smoking is rarely tolerated in white-collar workplaces. Half of all states prohibit smoking in offices, restaurants, and bars. In hundreds of parks and beaches throughout the country, smoking is verboten. Among college-educated, upper-middle-income Americans, tobacco addiction is far from the epidemic it once was. Most of them don’t smoke, and neither do their friends. In those circles, the problem may seem to have been solved.
The problem has not been solved, however. Forty-five percent of all Americans who completed a GED continue to puff away. The habit also persists for over 30 percent of American Indians and Alaska Natives. Perhaps most vexingly, smoking is rampant among the nearly 40 percent of the population with diagnosable psychiatric disorders; they smoke at a rate almost double the national average. Cigarettes continue to claim the lives of 480,000 Americans each year, accounting for one of every five deaths in America.
To put these numbers in perspective, consider the Pink Ribbon campaign that has mobilized millions of Americans to contribute to the battle against breast cancer. It’s a worthy battle by any measure. Yet how many people, even highly educated people, realize that 82 percent more American women now die of lung cancer than die of breast cancer?
Why is there no Brown Ribbon campaign to combat cigarette smoking? We fear that the answer lies in the fact that smoking is largely a low-income problem, and the resulting illnesses and deaths are often blamed on the victims. In certain circles, cigarettes are not only common but practically ubiquitous. Yet for those who run the nation’s businesses, those who shape its policies, those who fundraise, blog, and tweet, those who read and vote in the highest numbers, the issue has largely disappeared from view.
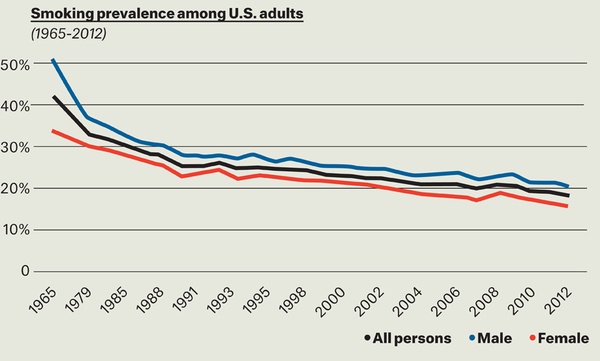
It took 40 years—from 1965 to 2005—to halve the rate of cigarette use. Today, somewhere in the range of 18 to 20 percent Americans smoke, depending on which national survey one reads. Will it take another 40 years for the rate to halve again?
It looks that way, based on a model one of us (Warner) has been developing with the University of Michigan’s David Mendez. The model, which we’ve been testing since the 1990s, has proven quite accurate thus far. Its predictions are sobering. Based on the rates at which people start and stop smoking—the latter hasn’t changed much in decades—it will take us until 2050 to come close to a national smoking prevalence of 10 percent. Ten percent sounds pretty good in light of both history and today’s numbers. But consider that 10 percent prevalence in 2050 implies that there will be hundreds of thousands of entirely preventable premature deaths from smoking every year.
Unfortunately, it will not be enough for public health professionals to push harder for the same approaches that have worked so far. The decline of the past few decades has largely been accomplished through mandating smoke-free workplaces in half of all states, increasing cigarette excise taxes in nearly all states, mounting effective media campaigns, and imposing restrictions on tobacco company marketing. To cut smoking prevalence in half again in fewer than 40 years will take something more than these evidence-based tools of the trade.
What is that “more”? The answer depends on whom you consult. Simplifying considerably, one can roughly divide the tobacco control community into three groups. The solutions championed by each group are not mutually exclusive, although listening to their most ardent proponents you might be forgiven for thinking so. As we will see, none of them can solve America’s smoking problem on their own. Collectively, however, they may have found the answer. They just don’t know it. These groups are the Traditionalists, the Harm Reductionists, and the Endgamers.
The Traditionalists are the largest group within the tobacco-control community. These veterans of the tobacco wars witnessed the remarkable progress wrought by the arsenal of evidence-based interventions noted above. These weapons have been able to beat back a tobacco industry that uses its economic might to pull strings in Congress and every state legislature. While the giant has not yet been slain, it has suffered serious wounds.
The Traditionalists believe that if we just do more with these
weapons, we will continue to achieve remarkable progress. They want to
jack up cigarette prices higher and higher, push the 20-some laggard
states to adopt smoke-free workplace laws, and extend smoke-free
coverage to public parks, beaches, university campuses, and public
housing. They want to see more large, creative, counter-advertising
campaigns like the CDC’s Tips From Former Smokers, in which real
people share their cigarette-related horror stories.
All of these approaches have been proven to work. Traditionalists often
point to California, one of the first states to adopt these measures,
where smoking prevalence now stands at 12.6 percent, the lowest in the
nation outside of Mormon Utah. In New York City, another oft-cited
example, former Mayor Michael Bloomberg made aggressive use of these
traditional tools, driving smoking down rapidly and substantially among
both teenagers and adults.
Traditionalists must face a discomfiting fact, however. These
conventional interventions will continue to bring progress—but
slowly, and only up to a point. Substantial tax increases, one of the
most effective interventions so far, eventually will come up against a
political and moral stone wall: the inequity associated with a
regressive cigarette tax. The majority of smokers are poor. They are
more price-sensitive than the rich, and when they’re confronted
with higher prices, they do quit in larger numbers than wealthier
smokers do. But whether rich or poor, only a minority of smokers quit
because of increased costs. That means most poor smokers continue to
smoke when the cigarette tax goes up, and the financial burden they
bear as a result is heavy indeed. So while we would like to see high
overall prices on cigarettes, there are clear limits to this approach.
Consider a married couple with a $30,000 a year income. If each spouse
smokes a pack a day and they live in a state where cigarettes cost an
average of, say, $6.00 a pack, they will devote 15 percent of their
very limited income to cigarettes. Six percent of their income will go
to cigarette taxes alone. If they live in New York City, the
city’s new minimum price per pack of $10.50 will drain a full
quarter of their income. Some low-income New Yorkers surely pay more in
tobacco taxes than they do in taxes to support Social Security and
Medicare.
Other evidence-based weapons in the Traditionalists’ arsenal have
limits, too. Half of all states already mandate smoke-free workplaces;
in other states, individual businesses have established smoking bans as
a matter of company policy. There are only so many more workplaces that
can go smoke-free. Some states have adopted additional smoke-free
policies—for instance, banning smoking in cars when kids are
present. But to bring about a huge leap in progress, such policies
would have to extend well beyond their current and readily defensible
limits. Smoking might have to be banned on all city streets, for
example, and perhaps even in non-workplace private properties like the
home, a proposition no one but a handful of
Prohibitionists/Abolitionists would support (more on them later).
Large counter-advertising campaigns constitute another major
evidence-based intervention. These require (and deserve) substantial
funding and virtually constant creative renewal. Fortunately, this year
will witness a barrage of tobacco control media campaigns coming from
the federal Office on Smoking and Health, the Food and Drug
Administration, and the American Legacy Foundation. But how long will
cash-strapped federal agencies be able to fund such programs? Even now,
the American Legacy Foundation is digging into its endowment to fund
its campaign.
The latest innovation in tobacco control—large graphic warning labels—should have festooned cigarette packs in September 2012. But their adoption was forestalled by industry legal action. If these labels do eventually become law, research suggests that they will decrease smoking, but the benefits may prove modest. And the ever-resourceful cigarette industry—and resourceful smokers—can always find ways to hide these unpleasant reminders, for example by repopularizing the old-fashioned cigarette case.
Harm reduction is simple in concept but controversial in practice. Instead of eliminating a given risky behavior, proponents of this idea seek to reduce the dangers involved—often by substituting a closely related, less-dangerous behavior. Examples abound: Offer chronic heroin users clean needles and methadone treatments. Instead of requiring abstinence-only education, teach students about birth control and, in some school jurisdictions, provide free condoms.
We know from research that many of these approaches work. Provision of clean needles has markedly slowed the spread of HIV in many nations. The designated driver campaign, perhaps the most successful contemporary use of harm reduction, has substantially reduced traffic fatalities by addressing drunk driving rather than alcohol consumption itself.
Some cigarette smokers very much want to quit, often desperately so, but simply find complete deprivation intolerable. Enter tobacco harm reduction (THR), the idea that some smokers can wean themselves off cigarettes—by far the most dangerous form of tobacco consumption—by switching to alternative nicotine or tobacco products.
Many anti-smoking advocates view such approaches with extreme skepticism. The two most prominent “harm reduction” efforts—created by the tobacco industry itself—caused tremendous harm.
The first was the filtered cigarette, which accounted for just 1 percent of all cigarette sales in 1950. That was the year the first scientifically robust study identified smoking as a cause of lung cancer. When these findings were publicized in the media—most notably in a December 1952 Reader’s Digest article entitled “Cancer by the Carton”—the first widespread smoking-and-cancer scare enveloped the nation. Smoking rates plummeted for two years as people scrambled to quit.
The industry responded by producing and heavily advertising filtered cigarettes, claiming that they let the flavor through while trapping the “bad stuff.” (The industry never specifically admitted that smoking caused lung cancer, or any other disease.) Kent, the first successful brand of filter-tipped cigarettes, was promoted as “the one cigarette that can show you proof of greater health protection.” It utilized an “exclusive Micronite Filter” that, ironically, was made of crocidolite asbestos.
Industry documents, subsequently made public as a result of tobacco lawsuits, reveal that the industry never truly viewed filtered cigarettes as less dangerous than unfiltered cigarettes. Rather, it viewed the filtered cigarette as a means of assuaging the public’s fears. Still, many people fell for the sales pitch, desperately seeking reassurance that it was okay to smoke. Smoking resumed its upward trajectory in 1955, and by 1960, filtered cigarettes dominated the market.
People did not smoke like the machines, however, and the industry knew it. Smokers held the cigarette in the middle of the filter tip, thereby occluding half of the ventilation holes. Smokers with large lips, referred to in the trade as “congenital hole-blockers,” might cover 100 percent of the perforations. For flesh-and-blood smokers, tar and nicotine yields were considerably higher than those recorded by the government’s testing machines.
Once again, industry documents show that low t/n cigarettes were public relations devices, designed from the beginning to allay the public’s fears. One prominent 1975 ad for True cigarettes shows a woman reflecting, “I thought about all I’d read and said to myself, either quit or smoke True. I smoke True.” These ads worked fabulously: Millions of Americans switched to low t/n cigarettes, many likely in lieu of quitting.
Most smokers found the low t/n product less satisfying than full-strength cigarettes. Struggling to get their accustomed levels of nicotine, low t/n smokers engaged in all kinds of compensatory behaviors, puffing harder or more frequently on their cigarettes, smoking them closer to the butt, and smoking more of them.
In a 1983 study, levels of cotinine, a derivative of nicotine, in smokers’ blood showed little to no correlation with the machine-measured nicotine yields. Smokers of low t/n cigarettes displayed lung cancer rates similar to those among people who smoked regular-yield cigarettes. The only real difference was that low t/n smokers developed cancers further down into the lung, apparently as a result of drawing harder on their cigarettes.
Thus, the two most successful entrants into the “harm reduction” market were not harm-reducing at all. Quite the opposite: They offered an attractive way to continue smoking to millions of frightened smokers who otherwise might have quit.
In the 1980s, R.J. Reynolds did attempt to market an apparently genuine lower-risk alternative to cigarettes, investing hundreds of millions of dollars in a product called Premier. Designed to look like a cigarette on the outside, Premier really was tobacco rocket science for its era. Small beads impregnated with nicotine were enclosed in an aluminum capsule inside the rod of the device. When the user lit the carbon tip with a cigarette lighter (because a match didn’t burn hot enough to ignite it) and sucked on the “filter tip” end, the heat evaporated the nicotine on the beads, allowing the user to inhale nicotine and glycerine.
The aluminum capsule was held in place by tobacco, even though no tobacco was actually consumed. The patent, which described the product as a nicotine-delivery device, noted that the tobacco in the product was optional; the capsule could have been held in place by any number of other means. Apparently the purpose of including the tobacco was legal: The device looked like a cigarette on the outside and included tobacco inside; therefore, the industry could argue that it was a cigarette (even if it wasn’t) and should thus be exempt from the usual FDA drug delivery device regulations.
Premier failed to impress consumers when RJR test-marketed it in 1988. Six years later, RJR test-marketed a similar product called Eclipse, which used a simpler system designed to generate a more pleasing taste and smell. That failed, too.